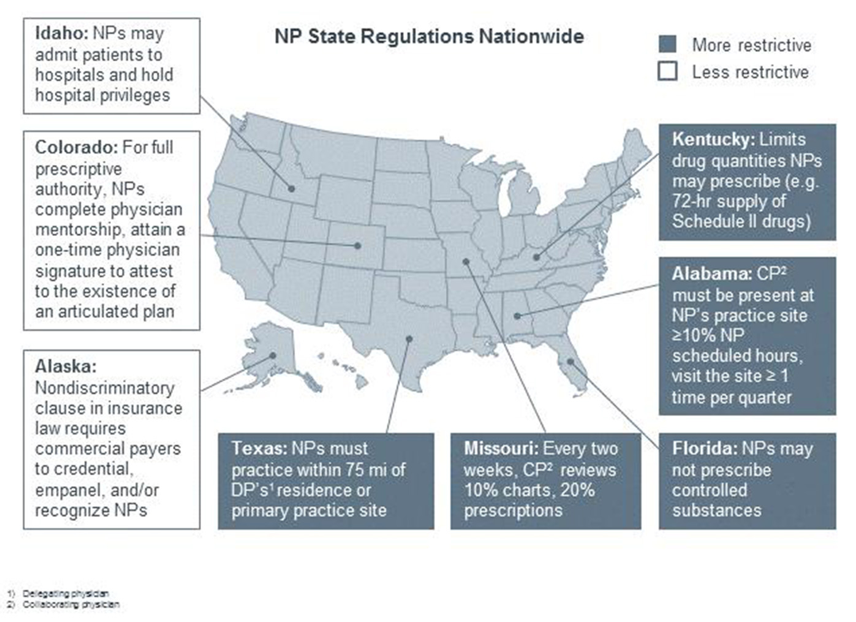
 ABSTRACT Nurse Practitioners (NP) should be allowed to practice medicine independently without physician supervision because they are well qualified and suited to provide much-needed primary care, especially to residents in rural and underserved areas. The looming shortage of physicians, upward spiraling healthcare costs, the chronically ill and millions of newly insured by the Patient Protection Act (PPA) and the Affordable Care Act (ACA), have led to a surge in new NP led facilities. Currently 17 states allow NPs to practice independently; however, NPs are gaining legislative momentum as studies show patients are seeking high quality, low cost, accessible care. Still, organizations such as the American Medical Association (AMA) and American Academy of Physicians (AAFP) and other physician groups have vigorously opposed such autonomy. The Federal Trade Commission (FTC) has even had to step in to ensure that opposition is warranted and because not physicians and others with special interests want to thwart competition. BACKGROUND History and Overview - Nurse practitioners are the principal group of advanced practice nurses (APRN) delivering primary care in the United States and they are often the initial point of contact for patients in many settings.1 An APRN has completed coursework and clinical education beyond that required of the generalist registered nurse (RN). All NPs must complete a master’s or doctoral degree program and have advanced clinical training beyond their initial professional RN preparation. The NPs gain clinical competency and specialized knowledge through didactic and clinical courses, this training equips them to practice in a variety of health care settings.2 Advanced-practice RNs represent about 8 percent of the nursing workforce and encompass four distinct roles: nurse anesthetists, nurse-midwives, clinical nurse specialists (nurses with advanced knowledge and skills in the care of special patient populations based primarily in acute care settings), and NPs.1 According to the American Association of Nurse Practitioners (AANP), 89 percent of advanced practice RNs work in primary care- e.g. pediatrics, adult health, gerontology, or nurse midwifery. Of those in primary care approximately 49% specialize in family care. They provide high-quality care in all communities rural and urban and in various other types of settings, including hospitals, urgent care facilities, private offices, academic medical centers and military facilities.4 They diagnose and manage acute and chronic conditions, with an emphasis on disease prevention and holistic health promotion. 4 There are more than 192,000 NPs practicing in the United States, with a projected total of 224,000 by 20155 and they treat over 916 million patients per year.3 Today the NP educational curriculum has advanced to provide more comprehensive clinical training and now offers the “Doctor of Nursing Practice” (DNP)6 at several universities across the country. In the treatment of their patients, NPs collaborate with physicians and other medical professionals as needed. This lends a certain high level of trustworthiness to the system of the autonomous practice. The first NP program began in 1965 because of a projected physician shortage.7 Under the direction of President Lyndon Johnson, Medicare and Medicaid were enacted and provided access to high-level health care to Americans who did not have health insurance, or who were locked out because of access and affordability issues. Under the Patient Protection and Affordable Care Act an estimated 32 million Americans will be newly insured and ready to access new health services. 8 NPs are licensed in all states and the District of Columbia, and practice under the rules and regulations of the state in which they are licensed. However, they face many regulatory restrictions in other states because of restrictive scope of practice laws. See Map: 9 On trend with the growing demand for primary care services because of the growing baby boomer population, the rise in multiple chronic care conditions and the newly insured under the ACA, this paper discusses the contributions and benefits of nurse practitioners in primary care and why they should practice autonomously across the United States. Nurse practitioners as primary care providers “Nurse practitioners are experts in health promotion, disease prevention, health education, and counseling as well as the diagnosis and management of common, and complex, acute and chronic diseases.” 1 The ACA focus on shared-savings and incentives for preventive care and wellness benefits for people who are already insured – will increase demand for primary care services. To manage the growing demand, the ACA calls for the expansion of nurse led centers and to include more autonomy for nurse practitioners. 10 The current primary care shortage in the country is staggering. An Association of Medical Colleges (AAMC)11,48 led study predicts a physician shortage of 90,000. A 2009 study by the National Association of Community Health Centers (NACHC) placed the number of individuals “lacking access to primary care” at 60 million.12 In addition, only 9 percent of US medical students are choosing family and general medicine, the two primary care services where the need is greatest. 13 Nurse practitioners have been offering high-quality, cost-effective, patient-centered health care especially to the aging population and in rural and underserved areas. 3 The ACA expanded Medicaid coverage but has also enrolled many people in high deductible insurance plans. 14 Many physicians do not accept Medicaid plans because of low reimbursements;15 rates NPs have done the opposite. Eighty-nine percent of primary care nurse practitioners report treating children covered by Medicaid as their primary coverage and most NPs report that they are currently accepting new patients with Medicaid. (AANP) The vast majority of NPs treat patients between the ages of 66 and 85 years; and 79% treat patients older than 85, making NPs well experienced to treat an aging population.3 The Nurse Practitioner: Incredible Resource for the Health Care System The NP is an incredible resource in our health care system - NPs are more than just health care providers; they are mentors, professors, advocates, and administrators. Their involvement in professional organizations and participation in health policy activities at the local, state, national, and international levels helps to advance the role of the NP and ensure that professional standards are maintained. There is thus no question they contribute significantly to the intellectual development of the medical profession. Their focus on health wellness and prevention has been undervalued, but public health officials and others in the medical community are starting to value prevention over too much technology and acute-care driven services.20 Lower Healthcare Costs – By providing high-quality care and counseling by focusing on a patients “functional, emotional, spiritual and mental health,”21 NPs can lower the cost of health care for patients. For example, patients who see NPs as their primary care provider often have fewer emergency room visits, shorter hospital stays and lower medication costs. 22 As patients become more cost-conscious about their health care costs, 17 utilizing a nurse practitioner will become a comparable, if not preferred choice. Studies that compared insurance claims from nurse practitioners and physician costs and retail clinics, showed that lower costs were associated with NPs. 18 In a study by the RAND Corporation on behalf of Massachusetts, the average cost of a visit to a NP was 20-35 percent lower than the average cost of a physician visit. 19 By substituting nurse practitioner visits for physician visits the analysis estimated statewide savings of $4.2-$8.4 billion for the period of 2010 – 2020. 1 If the nurse-managed healthcare center can be expanded out of the niche of an academic medical center and low-income populations20, this can translate into significant savings across the country if NPs can practice independently. In addition, emergency rooms have been proven to be an overcrowded and expensive way in which to care of the urgent needs of patients, especially those with chronic and complex diseases. 6 Nearly 51 million uninsured Americans seek care in the ED for minor issues that are nonurgent 27,28 Clinics run by nurse practitioners create cost savings by reducing the need for emergency rooms and hospitalization. 28 Patient satisfaction and outcomes- In a 2013 survey conducted by the Pew Charitable Trusts, more than six in 10 Americans supported giving more autonomy to NPs and seven out of 10 opposed regulations that would limit the patients choice to choose a NP as a primary care clinician. 21 A survey released in Medscape22 found that only 50 percent of physician patients reported that they felt doctors “always” listened carefully, compared with more than 80 percent of NP patients. There is a growing body of research that shows patients who were seeing NPs were more satisfied, had longer consultations, and had appropriate tests, with no appreciable differences in patient outcomes, processes of care or resource use. 1 Nurse practitioners were found to perform better on measures of patient follow-up; consultation time; satisfaction; and the provision of screening, assessment, and counseling. What makes NPs Uniquely Qualified to Act in the Stead of Physicians in Certain Situations “Nurse practitioners also function as a combination of a patient educator and a social worker,” says Anne Norman, DNP, FNP – AVP of AANP. Given the training and practice of NPs, they fit comfortably in the niche between physician and RN. They deliver a unique blend of nursing and medical care. What also sets the NPs apart from other health care providers is their unique emphasis on the health and well being of the whole person-the holistic approach to health and well being. They tend to focus on health promotion, disease prevention, and health education and counseling, NPs guide patients in making smarter health and lifestyle choices, which in turn can lower patients' out-of-pocket costs. Thus, the NPs are invaluable in the goal of a healthier society, because of their focus on holistic health, prevention, and cost effectiveness. NPs also have distinguished themselves from other healthcare providers by focusing on the whole person when treating specific health problems and educating their patients on the effects those problems will have on them, their loved ones and their communities. By providing preventative care, high-quality care and counseling, NPs lower the cost of health care for patients. Patients who see NPs as their primary care provider often have fewer emergency room visits, shorter hospital stays, and lower medication costs.27 Women’s health NP’s are even credited with improving communities, “we address a major healthcare need because if women are educated about themselves and what they need to do to take care of themselves, the result is a better community.” 23 Barriers for Nurse Practitioners Scope of Practice – Each state has a regulatory board that defines the “scope of practice” of medicine22 and these laws are the most significant barrier to nurse practitioners being able to work independently in the United States. In 17 states including the District of Columbia, NPs can practice medicine autonomously. In other states, regulations can impose complex and time consuming supervision requirements. In some states such as Missouri, collaborating physicians must review 10% of NP-provided care services and 20% of their prescriptions- both on a biweekly basis. 24 In Alabama, the collaborating physician must be present at an NP's practice site for at least 10% of the NP's scheduled hours.9 Not only can this disrupt the physicians’ schedule, especially in hard to reach rural areas, but also it is completely duplicative and inefficient since the NP is providing the same care as the physician. In Georgia, NPs are required to practice within a specified distance of their collaborating physician. 9 California and Ohio prohibit NPs from admitting patients to the hospital, disrupting the continuum of care. 9 In Missouri, one of the most restrictive scope of practice states, the costs of regulations are “overwhelming” even though the ratio of NPs to physicians are 3:1 and NPs could be providing much needed care in the many rural areas of the state. 24 The most important consequence of these state specific restrictions is at a cost to patient care. With a greater need to coordinate care, especially for the aging population, those managing complex medication schedules and in rural and underserved areas; the most vulnerable are often more affected. It can also deter nurse practitioners from working in states with a higher need, but more restrictions. With the provisions under the ACA expanding the role of nursing, and large agencies such as the Robert Wood Foundation supporting autonomous practice, the federal government will surely have a “a compelling interest in the regulatory environment for health care professions . . . especially that of APRNs,” asserted by the IOM.25 Payer policies restrictions – The payment policies of commercial health plans, Medicaid and Medicare vary considerably. These health plans can choose not to recognize NPs as primary care providers regardless of whether or not the NPs are the primary care provider. Plans can also decline to credential or pay NPs, which significantly constrains their practice. Surprisingly, under Medicare NPs are unable to order home health care or durable medical equipment. However, in certified Rural Health Clinics in medically underserved areas, NPs are recognized as primary care providers and reimbursed at the same rates as physicians.26 In 2013, Aetna changed its policy regarding reimbursements and now reimburses NPs at 85 percent of the physician rate. 27 The hope is for payers and the federal government to follow suit and increase reimbursement rates. If NPs are to practice in stand alone clinics, they must be able to earn enough revenue to support the facilities, equipment, supplies, salaries, etc. Although there is progress, nearly one-fourth of major health maintenance organizations (HMO) do not recognize NPs as primary care providers. These credentialing policies could diminish the ability of NPs to provide care to the most vulnerable populations and allow the denial of care because of poor reimbursement rates or no reimbursement at all. 28 Even when state laws are relatively permissive, payers may restrict NP practice by offering NPs lower rates than physicians, reimbursing them for fewer services, and denying them status as primary providers and direct billers. Because there is so much variation in scope of practice across states, payers and decision makers can adopt, out of simplicity, the most restrictive of standards for payment. States should work with payers to remove these restrictions, highlighting NPs’ impact on quality improvement and cost reduction. Physician Relations In a survey of 972 clinicians (NPs and PCP) 29 physicians reported working longer hours, seeing more patients and earning higher incomes than did nurse practitioners. NPs were more likely than physicians to believe that they should lead medical homes, be allowed hospital-admitting privileges, and paid equally for the same clinical services. The majority of physicians agreed that they provide higher-quality examination and consultations than do NPs during the same type of primary care visit, 75.3% of NPs disagreed. Physicians and NPs do not agree on the quality of care they provide. The Council of Medical Specialty Societies (CMSS), representing 34 physician organizations and 650,000 US physicians, and the American Academy of Family Physicians (AAFP) strongly oppose allowing expanding the scope of practice for advanced practice registered nurses.30 Some physicians also cite a “lack of data” and “well-designed studies”31 as reasoning not to expand scope of practice. The AAFP believes that the effort to expand scope of practice for APRN comes at the same time when the medical profession is embracing patient-centered medical home and “changing to an integrated, team-based approach.” 30 In another survey of NPs and physicians29 the majority of physicians agreed that nurses should practice to the full extent of their education and training but physicians were less likely to agree (17.2% physicians vs. 82.2% of nurse practitioners) that NPs should lead medical homes or be paid equally for the same services (3.8% physicians vs. 64.3% of nurse practitioners). Despite these results, there is evidence of collaboration on the ground, but more dialogue, organizational support and patient focused collaboration are needed. 32 Gaps in the Research - The advanced practice nurse led center is not a new concept, but the research is not as robust as compared to physician led centers. As urgent care centers surge in communities across the US,12 and having the first clinician point of contact be a nurse – more research will need to be done in regards to care coordination, patient satisfaction, and patient outcomes. Since growing minorities of NPs also practice in subspecialty areas, it will be of great interest to evaluate outcomes in these type of clinics and the patient demand and market response. The impact on health care costs in local communities, states and across the country should be evaluated. Lastly, data will be needed to see if the public knowledge and awareness of the NP profession has increased and whether or not the public can differentiate between nurse practitioners and physicians. ANALYSIS To keep the population healthy and lower health care costs, policy makers and medical experts will need to work together to change the way health care is currently delivered. One solid option is to standardize the scope of practice and licensure laws for nurse practitioners, allowing them to practice autonomously in the United States. Nurse practitioners have been practicing medicine and receive scores of equal to better care from patients. The expansion of nurse run facilities, in a study conducted by the RAND Corporation, 19 states that the physician shortage can be cut in half by 2025 without training another physician. It also found that investments in technology coupled with better care coordination could totally eliminate the physician shortage. In New York, Columbia Advanced Practice Nurse Associates (CAPNA) is a full service NP led primary care clinic in Midtown Manhattan, where NPs are paid equivalent pay for equal service. Managed by Nursing Faculty from Columbia University, CAPNA focuses on an, “emphasis on individualized disease prevention and health promotion.” 33 Thanks in part to the recent passage for the New York State Nurse Practitioner Modernization Act, NPs are authorized to practice independently without a written collaborative agreement with a physician. 34 As states continue to deal with the primary care shortage, this law passed by NYS, a state with equally great rural and urban areas, will surely be a model going forward. Importantly, interpersonal working relationships between NPs and physicians need to be improved. Although, a majority of physicians support the IOM report on the future of nursing, which states NPs should be able to practice to the full extent of their education and training. A majority of physicians did not support equal pay for the same services, nurses being full partners with physicians and nurse-led patient care. The IOM’s report countered this, stating NPs should have hospital admitting privileges, reimbursed at the same rate as physicians for providing the same service.16 NPs have expanded from working in just primary care settings to specialty and subspecialty roles such as oncology, women’s health and diabetic care.5 Not many research studies offer any substantial reasons to not allow NPs to practice autonomously or state that NPs provide inadequate primary care. Most of the opposition comes from physician groups such as the AMA and American Academy of Family Physicians (AAFP) whose chairman, Dr. Roland Goetz stated the profession was worried it was losing control of the word “doctor.” 35-36.In response, the AMA launched a “truth in advertising” campaign to help patients distinguish the difference between a physician and a non-physician “doctor.” 37 Nurse practitioners and physicians do not have to compete; both can deliver quality care to patients and have a positive effect on patients. 38 CONCLUSION It is unlikely that a majority of physicians will soon embrace the standardization of nurse practitioners scope of practice laws across the country. However, policy experts and the ACA calls for changing the way in which medicine are delivered, focusing on patient care and patient centered medical homes. Graduate rates in nurse practitioner programs don’t show any slow down and advocates for primary care and the NP practice are persistently lobbying for standardization of these laws. Valid concerns exist whether or not NPs can be profitable in stand alone clinics if payers do not reimburse at sustainable rates. 41 Patients have agreed that that NPs deliver equivalent, if not better primary care than physicians and with the growth in retail clinics, especially led by major brands like CVS, Kaiser39 and Wal-Mart,40 and with a lower cost, patients will be encountering NPs frequently. It seems inevitable that the demand coupled with the high skill and holistic care provided by NPs, they would be able to achieve the gold standard in all states to practice independently. REFERENCES 1. Naylor MD, Kurtzman ET. The role of nurse practitioners in reinventing primary care. Health Aff (Millwood) 2010;29:893-9 2. "Nurse Practitioner Role in Family Care Partnership." Web. 11 Dec. 2014. <http://www.dhs.wisconsin.gov/ltcare/partners/infoseries/rs11-07.pdf>. 3. AANP – What’s an NP? American Association of Nurse Practitioners. N.p., n.d. Web 11 Dec. 2014 http://www.aanp.org/all-about-nps/what-is-an-np 4. 30. Morgan PA, Abbott DH, McNeil RB, Fisher DA. Characteristics of primary care office visits to nurse practitioners, physician assistants and physicians in the United States Veterans Health Administration facilities, 2005 to 2010: a retrospective crosssectional analysis. Human Resources for Health (http://www.human-resources-health.com/content/10/1/42). 5. Ruegg, T “A nurse practitioner-led urgent care center: meeting the needs of the patient with cancer.” Clin J Oncol Nurs. 2013 Aug 1;17(4):E52-7. doi: 10.1188/13.CJON.E52-E57. 6. "Breaking: Mundinger to Step down as School of Nursing Dean." Columbia Daily Spectator. Web. 11 Dec. 2014. <http://columbiaspectator.com/2009/03/27/breaking-mundinger-step-down-school-nursing-dean>. 7. Mitchell, Charles, and Robert Spinelli. "Medicare Reform and Primary Care Concerns for Future Physicians." The Journal of the American Osteopathic Association 113.10 (2013): 776-87. Web. 8. About the Law. Healthcare.gov. Accessed 1 Dec. 2014.. http://www.healthcare.gov/law/about/index.html 9. "A Guide to Understanding State Restrictions on NP Practice." The Advisory Board Company. N.p., n.d. Web. 11 Dec. 2014. 10. 42 U.S.C. 6A: Public Health Service. 11. American Association of Medical Colleges. (2012). Recent studies and reports on physician shortages in the U.S. Retrieved from https://www.aamc.org/download/100598/data 12. "The Case for Urgent Care." Http://www.ucaoa.org/. 1 Sept. 2011. Web. 1 Dec. 2014. 13. National Resident Matching Program www.nrmp.org 1 Dec. 2014. 14. Wharam, J. F., F. Zhang, B. E. Landon, S. B. Soumerai, and D. Ross-Degnan. "Low-Socioeconomic-Status Enrollees In High-Deductible Plans Reduced High-Severity Emergency Care." Health Affairs (2013): 1398-406. Print. 15. Ollove, Michael. "Are There Enough Doctors For The Newly Insured?" Kaiser Health News Are There Enough Doctors For The Newly Insured Comments. 3 Jan. 2014. Web. 11 Dec. 2014. <http://kaiserhealthnews.org/news/doctor-shortage-primary-care-specialist/>. 16. "The Future of Nursing: Leading Change, Advancing Health - Institute of Medicine." The Future of Nursing: Leading Change, Advancing Health - Institute of Medicine. 5 Oct. 2010. Web. 11 Dec. 2014. <http://www.iom.edu/Reports/2010/The-Future-of-Nursing-Leading-Change-Advancing-Health.aspx>. 17. Mehrotra A, Liu H, Adams JL, Wang MC, Lave JR, Thygeson NM, et al. Comparing costs and quality of care at retail clinics with that of other medical settings for 3 common illnesses. Ann Intern Med. 2009; 151(5):321–8 18. Thygeson, M., K. A. Van Vorst, M. V. Maciosek, and L. Solberg. "Use And Costs Of Care In Retail Clinics Versus Traditional Care Sites." Health Affairs 27.5 (2008): 1283-292. Web. 19. Eibner, E et al. (2009). Controlling Health Care Spending in Massachusetts: An Analysis of Options. RAND Health. 20. Coddington J. (2010) Quality of Care and Policy Barriers to Providing Health Care in a Pediatric Nurse-Managed Clinic. Journal of Pediatric Healthcare, 24 (5):e9 21. Vestal, Christine. "ACA Medicaid Expansion Hurts Physician Shortage, Empowers Nurses -- Stateline." 19 July 2013. Web. 11 Dec. 2014. <http://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2013/07/19/nurse-practitioners-slowly-gain-autonomy>. 22. Crane, Mark. "NPs Top Physicians in Small Patient Satisfaction Survey." Medscape Medical News. 27 July 2011. Web. 11 Dec. 2014. <http://www.medscape.com/viewarticle/745381>. 23. Fontenot, Holly, and Joellen W. Hawkins. "The Evolution of Specialists in Women's Health Care across the Lifespan: Women's Health Nurse Practitioners." Journal of the American Academy of Nurse Practitioners 23.6 (2011): 314-19. Web. 24. Kliethermes, Jill. "ADVANCED PRACTICE REGISTERED NURSES SCOPE OF PRACTICE IN MISSOURI." 1 Jan. 2012. Web. 12 Dec. 2014. <http://www.doctorsofnursingpractice.org/documents/2012KliethermesPPT.pdf>. 25. Iglehart, John K. "Expanding the Role of Advanced Nurse Practitioners — Risks and Rewards." New England Journal of Medicine 20.368 (2013): 1935-941. Print. 26. American Medical Association (AMA), AMA Scope of Practice Data Series: Nurse Practitioners, Chicago, Ill. (October 2009). 27. (APRNs a "Big Part of the Solution" to the Primary Care Provider Shortage - Robert Wood Johnson Foundation) 28. (Population Health Management 2013;16:306–309) 29. Donelan, Karen, Catherine M. Desroches, Robert S. Dittus, and Peter Buerhaus. "Perspectives of Physicians and Nurse Practitioners on Primary Care Practice." New England Journal of Medicine 368.20 (2013): 1898-906. Web. 30. "CMSS RESPONSE TO THE FUTURE OF NURSING REPORT." Web. 11 Dec. 2014. <http://www.cmss.org/uploadedFiles/Site/CMSS_Policies/IOM FON Report CMSS Response.pdf>. 31. Chen, Pauline. "The Gulf Between Doctors and Nurse Practitioners." The New York Times 27 June 2013. Web. 2 Dec. 2014. 32. How to foster interprofessional collaboration between physicians and nurses? Incorporating lessons learned in pursuing a consensus. Princeton, NJ: Robert Wood Johnson Foundation, January 2013. 33. CAPNA http://www.cumc.columbia.edu/patient-care/findhealthcare#sthash.5MqOWmeK.dpuf 34. "S6356D-2013 - NY Senate Open Legislation." Web. 11 Dec. 2014. <http://open.nysenate.gov/legislation/bill/s6356d-2013>. 35. 25. Harris G. Calling more nurses ‘doctors,’ a title physicians begrudge. New York Times. October 2, 2011:A1. 36. Beck, Melinda. "Battles Erupt Over Filling Doctors' Shoes." Wall Street Journal. 4 Feb. 2013. Web. 12 Dec. 2014. <http://www.wsj.com/articles/SB10001424127887323644904578271872578661246>. 37. Truth in advertising campaign. Chicago: American Medical Association, 2010. 38. Garment, Victoria. "Nurse Practitioners and Physician Assistants: Why You Should Hire One (or the Other)." The Profitable Practice Blog. 31 May 2013. Web. 3 Dec. 2014. <http://profitable-practice.softwareadvice.com/nurse-practitioners-and-physician-assistants-why-you-should-hire-one-or-the-other-0513/>. 39. Luthra, Shefali. "Win-Win? CVS Joining Forces With Hospitals, Doctors." Kaiser Health News WinWin CVS Joining Forces With Hospitals Doctors Comments. 24 Sept. 2014. Web. 11 Dec. 2014. <http://kaiserhealthnews.org/news/cvs-medstar-team-on-electronic-medical-records-coordination/>. 40. Appleby, Julie. "The Walmart Opportunity: Can Retailers Revamp Primary Care?" Kaiser Health News The Walmart Opportunity Can Retailers Revamp Primary Care Comments. 17 Nov. 2011. Web. 11 Dec. 2014. <http://kaiserhealthnews.org/news/walmart-opportunity-can-retailers-revamp-primary-care/>. 41. Auerbach, D. I., P. G. Chen, M. W. Friedberg, R. Reid, C. Lau, P. I. Buerhaus, and A. Mehrotra. "Nurse-Managed Health Centers And Patient-Centered Medical Homes Could Mitigate Expected Primary Care Physician Shortage." Health Affairs: 1933-941. Print.
2 Comments
I've had a personal affection for Denmark since I was a baby, when my mother brought me there to visit her sister-in-law and my two cousins. I will have to dig up the baby pictures for another post! In 2008, I reconnected with my cousins in Copenhagen and have made several visits since. I also spent my vacations in Denmark talking to citizens about the Danish healthcare system and making comparisons it to the U.S. healthcare system. The Danish system, undergoing changes of its own and leaning towards more cost-sharing for individuals, is a system that provides healthcare for all. Denmark healthcare system focuses around primary care first and then specialists visits. The U.S. has caught on, realizing that so many conditions can be prevented, treated and managed by prioritizing primary care. I had given this presentation to strategy leaders at a major hospital in New York. I wanted to give them fresh perspective and inspiration by presenting some information on Innovisits and the Danish healthcare system. Although, there are distinct differences between our healthcare systems, we can be inspired and bring some (big and small) innovations back from Denmark. I must say that I have been enamored with this word, "Innovisit." I first heard it from Diane Stover-Hopkins, a panelist on the Innovation and Technology panel at the Becker's Annual Revenue Cycle and IT conference in Chicago about 2 years ago. I always knew what an innovisit was but had never heard the term until the conference. In graduate school, I studied the Virginia Mason case of implementing the Toyota Production System from Japan and the creation of Health City Cayman Islands (HCCI), a partnership between Ascension Health and Narayana Hospital in India. After doing some digging, I found an article from HBR highlighting steps to bring outside innovations into healthcare. This fascinated me and I became excited about the concept because so often we hear about the "silos" in healthcare. The silos run deep. So, how do we over come this? Check out my presentation and shoot me an email if you would like to discuss more. |
Tsahia (like Tsunami - yes, the T is silent - Sa-hee-ah) is a healthcare enthusiast working to transform patient care for all of us while driving creative and innovative solutions with technology. 


Archives
March 2021
Categories |
 RSS Feed
RSS Feed